Cuba’s life expectancy matches the United States despite sanctions, revealing how universal healthcare outperforms profit-driven systems.
There is a number that does not care about ideology, that cannot be gamed by flag-waving or GDP statistics, that cuts through every abstraction about freedom and markets and exceptionalism and lands on the only question that ultimately matters: how long do people live?
That number is life expectancy, and for the country that calls itself the greatest on Earth, it delivers an unambiguous verdict.
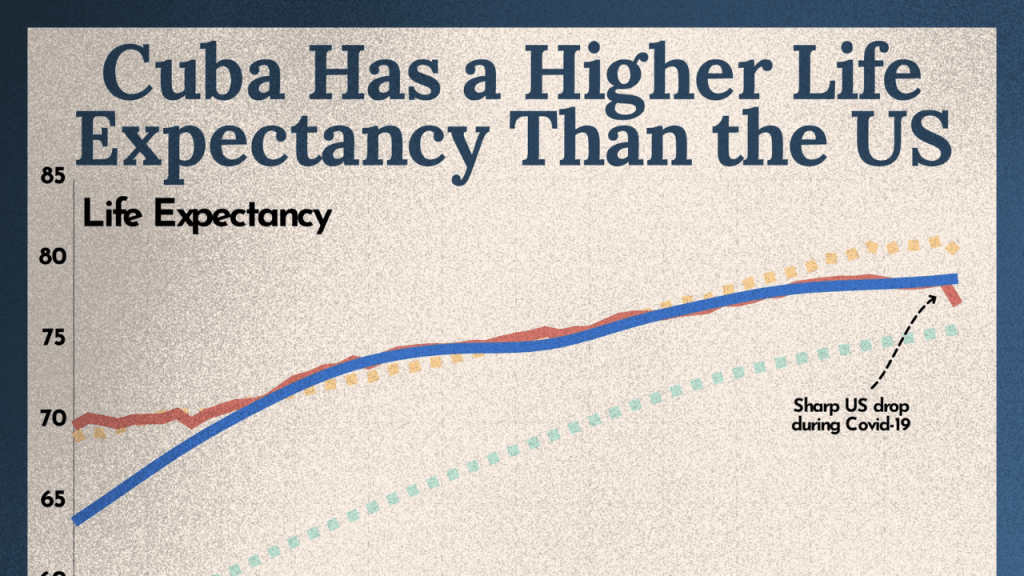
In 2019, before COVID exposed the architecture of every healthcare system on the planet, US life expectancy stood at 78.8 years according to the CDC. Cuba’s, according to PAHO data, stood at 78.3 years in 2024 — and tracked closely with the United States across the pre-pandemic period. A sanctioned island with a fraction of America’s per capita income had matched the richest country in the history of global capitalism on the most fundamental outcome a society can produce.
Then COVID hit, and the comparison became impossible to ignore. US life expectancy collapsed to 76.1 years in 2021, the sharpest two-year drop recorded since World War II, driven by preventable deaths, healthcare rationing, and the consequences of a system organized around extraction rather than survival. By 2023, despite a partial recovery to 78.4 years, the US still had not returned to its 2019 baseline — and remained 4.1 years behind comparable wealthy nations. Cuba absorbed the same pandemic under far worse material conditions, under tightened blockade, without access to the pharmaceutical supply chains or international credit markets the US takes for granted.
This is the data point that refuses to go away. And the reason it refuses is structural, not incidental.
Why This Metric Cuts Through Everything
Life expectancy is inconvenient precisely because it is unglamorous. It does not measure consumer choice, quarterly earnings, or the number of luxury hospitals in a metropolitan area. It measures something brutally simple: how long people live, on average, under a given social arrangement.
The number captures infant mortality, maternal health, workplace safety, chronic disease management, preventive care access, and the management of long-term illness. You cannot game it with world-class facilities available only to the wealthy. If large portions of your population are uninsured or priced out of care, the number falls. If chronic illness goes untreated because treatment requires financial ruin, the number falls. If a pandemic collides with a system that rations care by ability to pay, the number falls.
This is why defenders of American healthcare — when confronted with the data — pivot immediately to GDP, to “choice,” to abstract freedoms. Those are not responses to the metric. They are escapes from it. No freedom of consumer choice resuscitates the dead. No quarterly earnings report undoes preventable death. Life expectancy is the baseline verdict on whether a society is organized around human survival.
On that measure alone, the comparison is devastating.
How Cuba Produces These Outcomes
There is no mystery here, no ideological magic, no special cultural factor. The explanation is structural and unglamorous.
Cuba treats healthcare as infrastructure rather than commodity. Every citizen has access to care as a right, not a purchase. Doctors are embedded directly in neighborhoods, assigned to specific communities, and evaluated on prevention as much as treatment — creating continuous contact between providers and patients long before emergencies arise. The polyclinic system, linking community medicine to specialist care, functions as the spine of the entire health architecture.
The resource investment behind this is extraordinary on a per-capita basis. Cuba has the highest doctor-to-population ratio in the world — approximately 9.4 physicians per 1,000 people as of 2021, compared to 2.6 per 1,000 in the United States. This is not wealth producing this ratio. It is political choice. Cuba chose to train doctors at scale and deploy them where people live, not where profits are highest. The result is a density of clinical contact that no market-based system operating on profit incentives would produce, because the populations most in need of that density — rural areas, the elderly, the chronically ill — are precisely those least profitable to serve.
The same logic extends to research. Under an embargo that restricts access to equipment, financing, and pharmaceutical inputs, Cuba developed a domestic biotech sector oriented around public need rather than patent profit. The clearest example is CIMAvax-EGF, a therapeutic cancer vaccine developed by Havana’s Center of Molecular Immunology and made available to Cuban patients free of charge since 2011. The vaccine works by triggering the immune system to produce antibodies against epidermal growth factor — a protein that many cancers, including non-small cell lung cancer, require to grow. By depleting circulating EGF from the blood, it denies tumors a key mechanism of proliferation. A Phase III clinical trial published in Clinical Cancer Research demonstrated particular benefit in patients with high pre-treatment EGF serum levels, and a real-world Phase IV trial administered through 119 community polyclinics confirmed its safety and effectiveness in patients with no other treatment options. Roswell Park Comprehensive Cancer Center in Buffalo — the only US institution with FDA clearance to conduct CIMAvax trials — has called it groundbreaking and committed $4 million in donor funds to advance it.
That this vaccine emerged from a sanctioned country manufacturing it at approximately one dollar per shot is not a footnote. It is the argument. Pharmaceutical innovation in the United States is organized around patents, investor returns, and drug pricing structures that routinely price life-extending treatments beyond the reach of patients who need them. Cuba organized its biotech sector around what its population required. The outcomes reflect the difference.
The material conditions shaping these outcomes — sustained economic warfare, embargo enforcement, and the political logic of the siege — are examined in depth across the Cuba analysis on this site.
The US Failure Was Not an Accident
The United States did not stumble into declining life expectancy. Its healthcare system performed exactly as designed.
Healthcare in the US is fragmented, privatized, and rationed by price. Access is tied to employment, insurance networks, and the ability to pay. Preventive care is systematically deprioritized because it is less profitable than intervention. Chronic illness is monetized at every stage. Administrative overhead that serves billing rather than patients consumes an estimated 34 cents of every healthcare dollar. The result is a system that spends more per capita on healthcare than any other country on Earth while producing worse outcomes than comparable wealthy nations — a gap of 4.1 years in life expectancy against peer countries that cannot be explained by any factor other than structural failure.
COVID did not create these conditions. It made them impossible to ignore. The pandemic collided with a system optimized for extraction and produced mass premature death concentrated precisely where the system’s design predicts it: among the uninsured, the poor, Black and Indigenous communities excluded from adequate care by both price and geography, and those with untreated chronic conditions that market medicine had no incentive to address preventively.
The defense that the US has world-class medical technology is accurate and irrelevant. World-class technology organized to serve those who can afford it does not produce population health. It produces excellent outcomes for the wealthy and statistical catastrophe for everyone else. The life expectancy number averages across all of them. The average tells the truth.
The US healthcare system’s structural failure is not an anomaly within capitalism but a predictable output of it — a pattern traced across the global capitalism analysis on this site.
The Freedom Dodge
At this point the argument usually shifts. Confronted with outcomes, defenders of the system retreat to abstraction: what about freedom? What about choice? What about the innovation that markets produce?
These questions function as escape hatches, not responses. They allow the discussion to be moved away from the metric that actually matters onto terrain where ideology can operate freely, unencumbered by data.
The move deserves to be named for what it is: a definitional game. Freedom is invoked selectively. Freedom from preventable death is not counted as freedom. Freedom from financial ruin due to illness is not counted as freedom. Freedom to receive cancer treatment regardless of insurance status is not counted as freedom. Only the formal freedom to choose between insurance plans — including the freedom to choose none and die earlier — registers in this accounting.
When the definition of freedom is expanded to include material conditions, the comparison shifts immediately. A Cuban facing a lung cancer diagnosis receives CIMAvax through the neighborhood polyclinic at no cost. An American facing the same diagnosis navigates an insurance authorization process, a deductible structure, and a pharmaceutical pricing system in which analogous treatments carry price tags that drive families into bankruptcy. The formal freedom to navigate that system is not freedom in any meaningful sense of the word.
The innovation argument is similarly hollow as a defense of outcomes. The US does produce pharmaceutical and medical innovation at extraordinary scale. That innovation is priced to serve investors and shareholders, not patients. The gap between what the innovation produces and who can access it is not a market imperfection. It is the market functioning as designed.
The freedom rhetoric deployed to deflect material comparison between the US and Cuba does not operate in isolation — it is one expression of a broader ideological architecture examined across the imperialism analysis on this site.
The Verdict the Numbers Already Gave
This is not an argument for declaring Cuba perfect. Cuba’s healthcare system faces real resource constraints intensified by decades of US economic warfare. Facilities suffer from equipment shortages tied directly to embargo restrictions. The COVID period produced genuine strain. The system’s achievements exist alongside those documented limitations.
What the evidence requires is something simpler: that the comparison be made honestly, with the correct metric, without the ideological escape hatches.
A country under siege, denied access to international credit and pharmaceutical supply chains, with a per capita GDP a fraction of the United States, organized its healthcare system around prevention, universal access, and the deployment of medical resources according to population need rather than profit potential. The outcome, measured on the only metric that cannot be gamed, is life expectancy that matches or exceeds the richest country on Earth — and held far more stable when that country’s system collapsed under pandemic pressure.
The United States organized its healthcare system around profit and produced avoidable death at mass scale, a trend visible long before COVID and dramatically confirmed by it.
Life expectancy is not propaganda. It is the residue of policy choices, accumulated across millions of lives, averaged into a single number that tells you, without editorializing, who a system is built for.
The dystopia, by this measure, is outliving the empire. The numbers have already given the verdict. The only question is whether the people living inside the empire are allowed to hear it.
Sources
- PAHO — “Cuba Country Profile, Health in the Americas” (2024): https://hia.paho.org/en/node/124
- CDC / National Center for Health Statistics — “Provisional Life Expectancy Estimates for 2021”: https://www.cdc.gov/nchs/data/vsrr/vsrr023.pdf
- CDC / NCHS — “NCHS Data Brief No. 521: Mortality in the United States, 2023” (December 2024): https://www.cdc.gov/nchs/data/databriefs/db521.pdf
- Peterson-KFF Health System Tracker — “How does U.S. life expectancy compare to other countries?”: https://www.healthsystemtracker.org/chart-collection/u-s-life-expectancy-compare-countries/
- Wikipedia — “CimaVax-EGF”: https://en.wikipedia.org/wiki/CimaVax-EGF
- Rodriguez et al. — “A Phase III Clinical Trial of the Epidermal Growth Factor Vaccine CIMAvax-EGF as Switch Maintenance Therapy in Advanced Non-Small Cell Lung Cancer Patients” (Clinical Cancer Research, 2016): https://aacrjournals.org/clincancerres/article/22/15/3782/79235/A-Phase-III-Clinical-Trial-of-the-Epidermal-Growth
- Frontiers in Oncology — “Safety and effectiveness of CIMAvax-EGF administered in community polyclinics” (December 2023): https://www.frontiersin.org/journals/oncology/articles/10.3389/fonc.2023.1287902/full
- Roswell Park Comprehensive Cancer Center — “CIMAvax Lung Cancer Vaccine”: https://www.roswellpark.org/cimavax
- World Population Review — “Doctors per Capita by Country 2026”: https://worldpopulationreview.com/country-rankings/doctors-per-capita-by-country
- Wikipedia — “Healthcare in Cuba”: https://en.wikipedia.org/wiki/Healthcare_in_Cuba
- PMC — “Thomas McKeown, Meet Fidel Castro: Physicians, Population Health and the Cuban Paradox”: https://pmc.ncbi.nlm.nih.gov/articles/PMC2645168/